

Common Finishing Mistakes
_
Top Orthodontic Finishing Mistakes to Avoid | A Guide by Dr. Jeffery Taylor
The Finishing Stage of orthodontics is a fine balance of both art and science, and can often be one of the most stressful aspects of an orthodontic case. Proper finishing techniques are critical to ensuring well-balanced occlusion and long-term stability.
Top 7 Case Finishing Mistakes to Avoid
1. Beginning the finishing stage prematurely
Your case should have all the basic tenants of the mechanics stage completed before you begin the finishing stage. Some things to achieve before progressing to the finishing stage are:
1. Class I cuspid
2. Spaces closed
3. Level curve of Spee
4. Proper overjet
5. Proper overbite
6. No rotations
It is not wise to start finishing until you accomplished the above items, which are roughly Andrews Six Keys to Occlusion:

Don't make this mistake:
Finishing was started before Class I was obtained on the left:

Don't make this mistake:
Finishing was started before the upper space was closed.
Note the parallelism problem in the 32 as well.
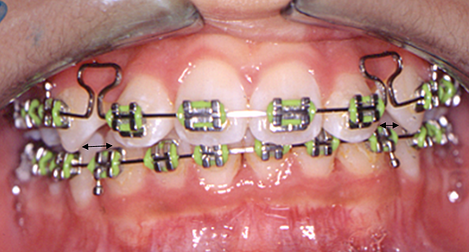
2. Expecting the custom (finishing) wire to correct minor rotations
Any rotations should have been corrected in the round niti phase since stainless steel wires do NOT correct rotations well. This isn’t due to a lack of skill of the operator, it is a problem related to the properties of the arch wire itself, regardless if you are using 018ss or 18x25 heat activated niti. Remember, if the bracket is straight to the wire but the tooth is not, it is best to change the bracket and then derotate.
Many times, the cuspid (upper or lower) may become rotated during the mechanics phase because it was not tied in properly during the retraction phase and/or extraction space closure. The ideal way to correct this is to return to the round niti and correct all rotations prior to starting finishing.

Don't make the mistake of rushing!
Make sure to correct this rotation before you start finishing
3. Failure to address the upper and/or lower 7s before you start wire bending
If the upper or lower 7s are NOT in alignment, we recommend you band and align them BEFORE you make any finishing bends.
In this example, the 7 was banded and will need to be aligned on a round niti since there are positional errors in all three planes of space.

4. Failure to make the wire return back to the same plane on a simple first order bend (up/down, in/out type bend)
Creating successful first order bends comes with experience. To minimize unwanted error, use the 1mm step pliers to make these simple bends. In the example below, you see a step down for the upper 5 and the plane for the 4 and the 6 are at different levels, creating a vertical change in the arch when none was desired.

5. Failure to make the bends be of an appropriate size
It is quite common in their first few orthodontic cases that doctors tend to make the bends too large when using the light wire plier. When this happens, the wire cannot be inserted, or the wire will bend and not deflect, or the bracket will debond. It takes practice to overcome this.
6. Failure to change archwire shapes to make the upper and lower fit together more ideally
Frequently, the upper arch will expand more than the lower arch which makes the incisors end to end and/or the upper space hard to close. If you’re experiencing these issues, you might want to consider changing the shape of the wires.
In the example below, the case is not yet in the finishing stage, however you can see that the upper is too wide by looking at the upper to lower cuspid relationship.
Here is the same case after tapering the upper and expanding the lower at the finishing wire phase of treatment. Note the cuspid relationship at this phase:

7. Entering the finishing stage without a plan
Without a finishing treatment plan, you will lack the precision and efficiency needed to finish the case correctly. With a bit of time spent on pre-planning, you’ll be able to:
· Reposition brackets to correct rotation and long axis errors
· Realign as needed on round or rectangular niti wires
· Maximize efficiency by placing 018ss and making ALL the bends needed at the same appointment.
· Maintain proper wire length by making your wire bends in a pre-planned order
· Ensure you address the 7s as needed
· Reduce your stress in the clinical setting
· Obtain the best finish possible for your patient

The Injuries That Weren't
RAWLE & HENDER SON LLP
In order to prove a case in dental malpractice, a plaintiff must demonstrate that there was negligence on the part of the dentist which directly caused, or was at least a substantial factor in causing, an injury or injuries. If any of those components is missing, the claim cannot stand; in other words, if there is no improper treatment, or if there are no demonstrable injuries, or if there is no connection between the treatment and the injuries, the dentist will be successful in defense.
F A C T S
A 45-year-old woman had been having pain associated with her lower right third molar (#32) for nearly a week; she had previously experienced the same problem over the years, but the pain resolved after a few days after an uptick in her oral hygiene. But this time was different. So, she went to her dentist, Dr. A, to complain, leading to a panoramic radiograph which showed the tooth to be partially impacted with a distal bony defect present on tooth #31, which was confirmed on clinical examination. Dr. A believed that extraction was the best treatment, given the history and the patient’s age; the patient was so uncomfortable that she was happy to hear that proposed solution.
Dr. A had spent several years working in hospitals, so he was well experienced with extractions of this type, and extractions became a regular part of his private practice. What was clear radiographically was the proximity of the root apices to the inferior alveolar canal, so the dentist carefully explained the potential for temporary, or even permanent, loss or alteration of feeling to the areas innervated by the inferior alveolar nerve. The patient was then presented with a detailed informed consent form, which she signed and dated before any aspect of treatment began. Later on, the patient acknowledged having been fully advised of all risks associated with the procedure, as well as viable options, so her initial case claim of lack of informed consent was dismissed by the court early on.
Under local anesthesia, tooth #32 was surgically extracted, seemingly without complication. During the
20-minute procedure, a bite block was placed on the contralateral occlusal surfaces to keep the masticatory muscles comfortable and to reduce the chance of TMJ injury. A silk suture was placed, post-extraction instructions were provided (including that she should refrain from smoking), and a prescription for analgesics was given.
On the second post-operative day, the patient experienced an increase in pain, so she called the dentist’s office; she was asked to come in to be checked, and she did so that afternoon. When Dr. A checked the area, he found a dry socket. So he asked the patient whether she had been smoking, and she admitted to having done so. The dentist gently debrided the socket, packed the area with dry socket dressing, reiterated the warning against smoking, and told the patient that she should return for dressing changes at least every other day. The patient made no other complaints related to her mouth at that visit.
The patient returned quite often for dressing changes, still making no other complaints; her suture was removed one week after the extraction. During the first month, she presented to the office 12 times for dressing changes. At one of those visits, the dentist took an x-ray, which showed a clean site. At 35 days following the extraction, the patient complained, for the first time, that her lower right lip and chin were numb; she stated that the numbness had been that way since the day of extraction. When asked why she had not said anything about that before, she responded that the pain from the dry socket had been so bad that she simply complained of the most significant thing. Dr. A gently used a sharp explorer to try to determine whether there was any painful response, but the patient stated that she felt nothing on her lower right lip and chin areas when poked with the explorer. The dentist wanted to follow that situation, so he had the patient return for continuing dry socket dressing changes, and after that resolved, once a month. He told the patient that, if she did not have a return of feeling by 6 months after the extraction, she would be referred to an oral surgeon.
At nearly 3 months post-op, she made a new complaint: she was experiencing left side TMJ pain (which she attributed to the bite block used at surgery) which was ongoing since the time of the extraction, and which was making it difficult for her to chew. The dentist thought that it was best that she be sent to an oral surgeon at this point, to address the complaints of both numbness and joint pain. The patient became
upset that she was being referred elsewhere, asking why Dr. A would do surgery if he was not able to handle post-surgery problems on his own. The dentist explained that he felt comfortable managing post-surgery problems, but when two arose at once, it would be better to have a specialist involved.
The patient never returned to Dr. A, and she ignored voicemails from his office asking whether she had gone to see an oral surgeon.
L E G AL S TAN C E
The patient became a plaintiff when the attorney she retained filed a dental malpractice action on her behalf: the suit alleged an improperly performed extraction during which the inferior alveolar nerve was not protected, improper use of a bite block, and the failure to obtain informed consent. These issues of malpractice were claimed to have caused permanent injury to the right inferior alveolar nerve (IAN) and damage to the left TMJ complex. (As is noted above, the informed consent claim dropped out of the case.)
IS S U E S R A IS E D
As we commonly see in cases claiming paresthesia due to extractions, the method of extraction is of paramount importance because a properly performed extraction which led to nerve injury is normally not an adequate foundation for a successful dental malpractice case. A less common claim was raised here, that being that it was improper to place a bite block during the extraction, so as to cause a joint injury.
D I S C OV E R Y
In the state where this suit was brought, there is broad discovery permitted by the courts, meaning that attorneys for both the plaintiff and the defendant dentist are allowed to delve into any issue(s) that might at least reasonably lead to relevant evidence. What this practically results in are the (1) depositions of the
plaintiff and defendant, as well as of key non-expert witnesses who can likely shed light on important issues of the case; (2) a physical examination of the plaintiff by a doctor of defense counsel’s choosing, which is limited to the damages claims; and (3) access to a generally wide array of the plaintiff’s dental and medical records, so long as defense counsel can demonstrate to the court that the records sought are not merely for a fishing expedition, but rather for an exploration of what the plaintiff might have reported – or not reported – to her seemingly unrelated medical providers.
Here, the plaintiff’s deposition was not overly helpful in areas beyond the usual inquiry into the plaintiff’s background and her version of the treatment timeline, including interactions with the defendant and others.
However, we had an oral surgeon who was familiar with issues relating to the TMJ and to nerve injuries examine the plaintiff. When challenged with various stimuli to the areas innervated by the IAN, she claimed that she could not feel the right side, but she could feel the left side; of course, this is subjective, so patient truthfulness is an important component of this type of examination (which is why we sometimes forego such examinations in claimed nerve injury cases, based upon how we view the plaintiff’s veracity). Regarding the claim of left-sided TMJ pain, she told our examining oral surgeon, and acted as such when asked to perform opening and lateral movements, that she could only open vertically to 25 mm when asked how wide she could open, but when the oral surgeon asked her (off-the-cuff, so to speak) to open so that he could view the back of the extraction site with a mouth mirror, she opened 45 mm without even a hint of discomfort. More importantly, regarding the left-sided TMJ pain, she claimed to be unable to move laterally, at all, to the left, but freely moved toward the right without any restriction. The written report of this examination was shared with counsel for the plaintiff, as is required.
What the plaintiff did not know is that, due to the functions and pulls of the lateral pterygoid muscles, patients are able to freely move toward the injured side, and prevented from moving to the opposite direction of injured TMJs. Without anyone intentionally setting it, the plaintiff fell into an anatomic trap, proving her to be untruthful regarding her TMJ claim, which immediately raised our awareness that, perhaps, she was also being untruthful about the nerve injury claim.
The plaintiff was a patient who saw doctors quite frequently, so the volume of medical records to be reviewed was enormous. However, we recognized that they could contain very valuable information. Roughly 18 months after the extraction at issue, the plaintiff saw her primary physician for a routine physical and blood studies: therein, her liver function tests were grossly abnormal, so her physician referred her to a hematologist for a work-up, and she went.
Luckily for us, and in conformity with good medical care, the hematologist obtained a complete medical history and conducted a thorough physical exam. In the history, within the section entitled “neurological”, the hematologist noted the history from the plaintiff, which included her statement of “no areas of numbness or altered sensation.” As helpful as that, alone, would have been for our case, during the physical exam, the hematologist conducted a neurological exam, in which it was noted “CNs (cranial nerves) II-XII intact.” Given that the IAN is within the third division of CN V, we knew, from a totally unrelated but authoritative source, that no nerve was injured, at least as of then.
Subsequently, and pursuant to a HIPAA authorization, we spoke with the hematologist. We explained the plaintiff’s claim in the suit and asked whether the notes of the history and physical were accurate. The
hematologist responded to the effect of, “I never enter a patient chart note that is not complete and accurate. I see almost every patient with either a medical student or resident also present, so complete history taking, thorough examinations, and accurate chart entries are absolutes.” We made plans to have the hematologist testify at trial, if needed.
T R IAL
In the lead-up to trial, we explained to the plaintiff’s attorney that we strongly believed that the claimed injuries did not exist. The attorney did not accept our assessment, maintained a settlement demand value which we viewed as exorbitant, and wished to proceed to trial.
At trial, our client testified regarding his professional credentials, including his practice background, and the facts specific to this plaintiff. A key area of questioning against him, which was effective, focused on the concepts that oral surgeons are specifically trained to remove impacted teeth. As compared with general dentists such as he was, they are more familiar with handling complications (which the dentist clearly agreed with, as he had ultimately referred the plaintiff to an oral surgeon after two problems emerged), and despite his experience doing oral surgery, an oral surgeon with more experience might have taken different approaches and precautions to decrease the likelihood of complications. In all candor, plaintiff’s counsel seemed to have impressed the jury on the negligence aspect of the claim.
However, things turned around starkly during the cross-examination of the plaintiff’s expert witness. That expert acknowledged the anatomic and physiologic incongruities associated with the plaintiff’s claimed limitations and abilities relating to her TMJ and its muscular attachments, and essentially admitted that the plaintiff could not have been truthful when reporting her TMJ symptoms. It became even worse for the plaintiff when the expert was confronted with the hematologist’s records, which he had never previously reviewed, and was forced to admit that this unbiased, unrelated practitioner had essentially debunked the
plaintiff’s claimed permanent nerve injury, based upon a history from the plaintiff and an examination which took place well after the subject extraction.
The jury quickly returned a verdict in favor of the dentist. One of the jurors, who was interviewed after, said that they completely disbelieved everything about the plaintiff’s claim once her own expert was painted into a corner.
TA K E AWAY S
For a plaintiff to win a dental malpractice case, every element of the claim must be met. So, an injury caused by proper treatment will lead to results in favor of the dentist. Of course, the true facts may not always appear from the start, so a deep dive into every aspect of litigation investigation must be undertaken in all cases, not only by the attorneys, but by the expert witnesses as well, because they are the witnesses who are usually the most critical to juries.
Very important from a risk management standpoint is the concept to always practice within your own abilities. Especially in office settings when young employee dentists are pushed to produce, but also in situations where such pressures are not externally placed, we often see litigation arising after dentists perform procedures for which they are not adequately trained, for which they have limited experience, or which they are trying to do as “a favor.”
medpro.com/dental
The opinions expressed through this post are the opinions of the individual authors and may not reflect the opinions of MedPro Group or any of its individual employees. This document should not be construed as medical or legal advice. Because the facts applicable to your situation may vary, or the laws applicable in your jurisdiction may differ, please contact your attorney or other professional advisors if you have any questions related to your legal or medical obligations or rights, state or federal laws, contract interpretation, or other legal questions. MedPro Group is the marketing name used to refer to the insurance operations of The Medical Protective Company, Princeton Insurance Company, PLICO, Inc. and MedPro RRG Risk Retention Group. All insurance products are underwritten and administered by these and other Berkshire Hathaway affiliates, including National Fire & Marine Insurance Company. Product availability is based upon business and/or regulatory approval and may differ among companies. © 2019 MedPro Group Inc. All rights reserved.

Unsuccessful Outcomes
Does a judge have to instruct the jury that a bad result, in and of itself, is not evidence of malpractice? This was the question that the court had to answer in Schuessler v Wolter,310 P.3d 151 (Colo. App., 2012). The plaintiff suffered from degenerative disc disease and a lumbar herniation. The defendant recommended 2 methods of treatment: the first, steroid injections, and the second, surgical intervention. The plaintiff ultimately chose the second option—surgical discectomy with subsequent fusion. Although the surgery itself was successful, the plaintiff postsurgically experienced chronic hypersensitivity and numbness of his right side, symptoms that were not present presurgically.
The plaintiff claimed that the defendant damaged his spinal cord during the surgery. The defendant claimed that the injury the plaintiff suffered was a known risk of undergoing the procedure even when reasonable care was used and can also occur even with an absence of negligence. The defendant requested that the court issue the following jury instruction. As to Plaintiff's negligence claim, a physician does not guarantee or promise a successful outcome by simply treating or agreeing to treat a patient. An unsuccessful outcome does not, by itself, mean that a physician was negligent.
The court refused to issue the instruction, and the jury found for the plaintiff after a 9-day trial, awarding the plaintiff just under 1 million dollars. This appeal then ensued. The appellate court noted at the outset that determining whether a trial court abused its discretion regarding not giving a requested jury instruction could only be found if (1) the court based its decision on an erroneous view of the law; (2) the court acted on an erroneous assessment of the evidence; or (3) the decision not to give a requested jury instruction, on review of the record, shows that the jury might have reached a different conclusion resulting in a different verdict.
Looking at prior case law on this issue, the appellate court noted that “a physician does not undertake to warrant a cure and is not responsible for want of success unless it results from a failure to exercise ordinary care” (Cit. Omit.). The reason that the law takes this position is, first, because the jury must be informed that a bad result, in and of itself, is not an indication that negligent treatment was rendered. Second, they must be made to understand that a bad outcome alone cannot be considered in determining whether a doctor has met or fell below a given standard of care. Citing another case to support this contention, the court noted that “a plaintiff may not rely solely on a bad outcome to prove liability, but must provide evidence that the physician failed to exercise reasonable care” (Cit. Omit.). The appellate court reversed the trial court's decision and remanded the case for a new trial.
Commentary
Clinical orthodontics is the perfect petri dish in which to examine this legal principle. The realities of clinical practice denote the fact that any number of our completed cases are finished with a less than successful outcome; some would call them bad results. On the other side, many would posit that orthodontics deals with making the abnormal normal; and normal is a range, not a point. We don't, and sometimes we can't, nail every case perfectly, and therefore, realistically, orthodontics doesn't deal with correction; rather, our strong suit is improvement. We make many things better, like smiles, bites, functionality, self-image, and the like. But hitting a home run every time we come up to the box, well, that's just not realistic.
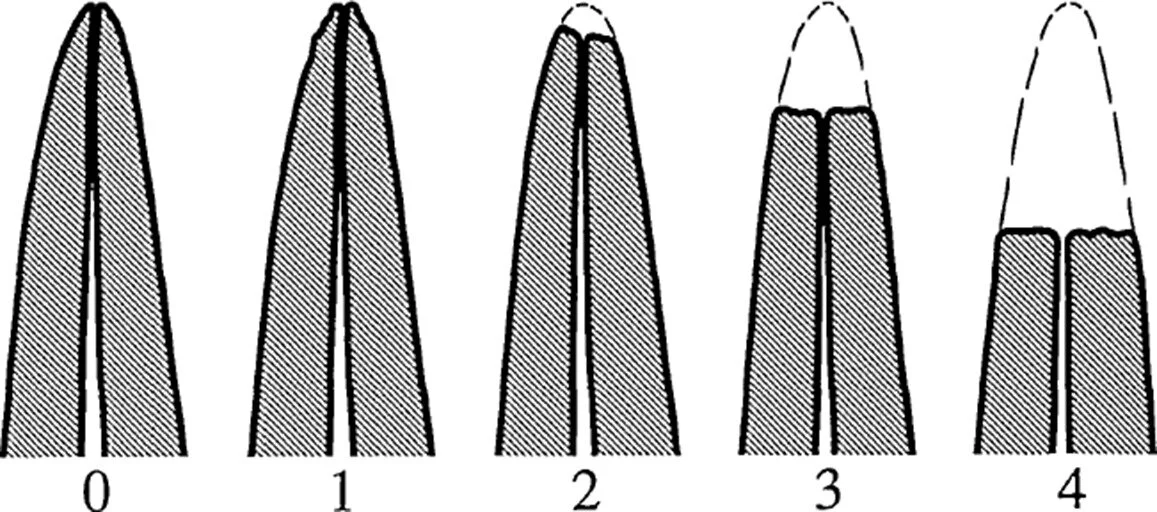
At the end of the day, we may not have achieved a solid Class I molar relationship, and I know some, no make that more than some, who would call that a bad result. The same goes if a few marginal ridges are not in perfect juxtaposition. Likewise, for a 3-4 mm overbite instead of a 1-2 mm vertical relationship. How sad to think of these as poor results.
Come to think of it, do we as a specialty really have a consensus as to what is and what is not a good result? We should, but we don't. The American Board of Orthodontics is on the right track as one can still pass on a given case with less than a perfect score. But because we want to nail every case, we often make excuses for our less than desirable outcomes, such as poor growth or a lack of patient cooperation. Therefore, if there are excuses, the results can be excused. If they can be excused, they can't be bad. Nope, no bad results for us. At this point, you should be asking, “C'mon Larry, what are you talking about?”
A good example is our current penchant for deluding ourselves that nonextraction therapy is a goal. It is not! Nonextraction therapy is merely a means to achieve a goal. Methodologically, we should first determine where we want the teeth, what angulation, proclination, articulation, inter- and intraocclusal relationship, A-P position, verticality, whatever. Once you decide where you want them, then you decide how to put them there. Maybe the way to get there is nonextraction via expansion, distalization, reproximation, what have you. Maybe the method might involve the extraction of any number of teeth using a symmetrical or asymmetrical pattern. Maybe it involves a multidisciplinary approach enlisting orthognathics, prosthetics, or orthopedics. The point is that these treatment modalities are the means to a desired and well-planned goal. No, many of us have deluded ourselves into drinking the nonextraction Kool-Aid. But hey, that's okay because 30 years from now, we'll have a built-in patient base of patients we have to re-treat. No big deal, as a specialty, we've done this once before.
Another example is the importance placed on obtaining a Class I molar relationship. Many of us have bought into the proposition that if the molars are not Class I, then our treatment has failed. Sorry, can't buy it. Many practitioners have decided that it’s okay to increase both treatment costs and time to themselves and their patients by using the multitudes of molar distalization appliances available on the market to push molars back into Class I; when instead, premolars could have been extracted, resulting in the same anterior segment positioning. If the goal is to obtain a mutually protected occlusion, one should be analyzing the safest, most expedient ways to achieve this end goal instead of maintaining a blind allegiance to a questionable anatomic tenet. If it's okay to substitute canines for lateral incisors, it's okay to take out maxillary premolars instead of distalizing everything.
I know, you have to compete with the guy down the block who genuflects to the misinformed helicopter parent or the guru de jour who is being compensated to tout the latest and greatest gizmo or widget. I get it. Sure, we're in a specialty, but it's also a business, and want it or not, we are in competition with our colleague down the block. Yet, it's sad to have to recognize one of our frailties; our relative inability to educate not only our patients but our referral base as well. Some would say we are on the verge of forgetting our own education in that we have traded a number of our principal principles all because we are afraid to lose a patient to a colleague.
What we need is some standardized means to evaluate our results, some type of outcomes assessment mechanism. We need a tool developed by our specialty not only for use by our rank and file but also for use by those who would seek to describe and evaluate our ministrations as successes or as unsuccessful outcomes. At the end of the day, it's important to remember that most of our treatment is very successful; it's just not perfect.

Clear Aligner Orthodontic Treatment and Root Resorption
During Dr. Prittinen’s course, we took some time to discuss root resorption using clear aligner therapy. I would like to elaborate on this topic. First, we need to distinguish between generalized and localized resorption. As you are probably aware and have probably seen in your own practices, some patients suffer from generalized resorption. These patients would be excluded from orthodontic treatment during the diagnostic phase. In contrast to severe generalized resorption, severe localized resorption involving a few teeth usually is caused by orthodontic treatment. It has been known for many years that excessive force during orthodontic treatment increases the risk of root resorption, particularly if heavy continuous forces are used. Prolonged duration of orthodontic treatment also increases the amount of resorption.
It is increasingly apparent that some individuals are more susceptible to root resorption. It seems reasonable to presume that the large individual differences relate to genetic factors, although there is not any way to use genetic testing to evaluate resorption risk. However, one way to screen for potential genetic factors relating to root resorption would be to simply ask the patient’s parents if they had braces and if they did, did they experience root “shrinkage”? As a reminder, our US Dental Institute pre-treatment evaluation always includes family history as it relates to growth, orthodontic treatment, extractions etc.
Our policy to detect those who are likely to experience unusually large amounts of resorption is to take a panoramic radiograph 6 to 9 months into treatment and evaluate the amount of resorption during this time. As Dr. Prittinen reminds the attendees at his lectures, this is also the standard of care as determined by the American Association of Orthodontists (AAO).
Patients who show significant resorption in the initial stage of treatment are likely to have greater resorption at the end of treatment. In my own experience, I have stopped treatment in a few cases where I anticipated that the crown root ratio would be adversely affected by continuing treatment. We also had patients in our practice that never completed orthodontic treatment due to resorption. Thankfully this is a rare occurrence.
This gets us to clear aligner orthodontic treatment and root resorption. To date, I know of no report in the literature involving clear aligner therapy and root resorption. This could be just good fortune or it may have something to do with the development and design of CA therapy. First, CA was initially designed for adults. It’s logical to assume that since tooth movement in adults is slower, then the programmed movement in aligners would reflect this. Currently Invisalign and Reveal use the following movements per aligner: 0.25 mm linear, 2 degrees rotation, 1 degree root torque. This was conservative since the original protocol called for a 14 day aligner cycle. Thus, the total movement per month was about half of normal expected orthodontic movement with fixed appliances and was self-limiting since each aligner had a maximum designed tooth movement and force. It seems that the engineering of aligners can be more precise than a fixed system where initial generated forces can be very large. This “division of force” may be the reason that there has not been a report in the literature involving CA therapy and root resorption.

Repositioning Of The Mandible & What Happens
Improved clinical use of Twin-block and Herbst as a result of radiating viscoelastic tissue forces on the condyle and fossa in treatment and long-term retention: growth relativity.
Understanding mechanisms of action for orthopedic appliances is critical for orthodontists who hope to treat and retain the achieved corrections in patients with initial Class II mandibular retrognathism. That knowledge can help orthodontists produce clinically significant bone formation and avoid compression at the condyle-glenoid fossa region. It also assists us to understand the differences between short-term and long-term treatment results. It was previously thought that increased activity in the postural masticatory muscles was the key to promoting condyle-glenoid fossa growth. By analyzing results from several studies, we postulate that growth modification is associated with decreased activity, which leads to our nonmuscular hypothesis. This premise has its foundation on 3 key specific findings: significant glenoid fossa bone formation occurs during treatment that includes mandibular displacement; glenoid fossa modification is a result of the stretch forces of the retrodiskal tissues, capsule, and altered flow of viscous synovium; observations that glenoid fossa bone formation takes place a distance from the soft tissue attachment. The latter observation is explained by transduction or referral of forces. Evidence is presented, therefore, that the 3 trigger switches for glenoid fossa growth can similarly initiate short-term condylar growth modifications because the 2 structures are contiguous. These are displacement, several direct viscoelastic connections, and transduction of forces. Histologic evidence further shows that stretched retrodiskal tissues also insert directly into the condylar head's fibrocartilaginous layer. The impact of the viscoelastic tissues may be highly significant and should be considered along with the standard skeletal, dental, neuromuscular, and age factors that influence condyle-glenoid fossa growth with orthopedic advancement. These biodynamic factors are also capable of reversing effects of treatment on mandibular growth direction, size, and morphology. Relapse occurs as a result of release of the condyle and ensuing compression against the newly proliferated retrodiskal tissues together with the reactivation of muscle activity. To describe condyle-glenoid fossa growth modification, an analogy is made to a light bulb on a dimmer switch. The condyle illuminates in treatment, dims down in the retention period, to near base levels over the long-term.
“ significant glenoid fossa bone formation occurs during treatment that includes mandibular displacement; glenoid fossa modification is a result of the stretch forces of the retrodiscal tissues, (stretching of the) capsule, and altered flow of viscous synovium”
- Voudouris and Kuftinec
The posterior, anterior, and lateral attachments of the retro- discal articular disc complex are shown. The condyle is usually guided upward and backward to CR by these and other attachments (from an open jaw position).
When the complex is pulled forward opposite to the direction of the arrows, glenoid fossa modification occurs. Studies have shown that not only the pull of these tissues lead to these changes, the altered dynamics of the synovial fluid facilitates growth beneath the hydrophilic condylar fibrocartilage. In the upper chamber, the opposing anterior flow of synovial fluids similarly influences glenoid fossa growth.
THREE GROWTH STIMULI WORK TOGETHER
Displacement + Viscoelastic tissue pull + Referred Force = Remodeling / Growth of bone in the Glenoid Fossa (along with some growth at the posterior superior aspect of the condyle)
The concept that viscoelastic tissue forces affect growth of the condyle and bone of the Glenoid Fossa suggests that modification first occurs as a result of the action of anterior orthopedic displacement.
Second, both the fossa and the condyle are affected by the posterior viscoelastic tissues anchored between the glenoid fossa and the condyle, inserting directly into the fossa and the condylar fibrocartilage.
Finally, it is hypothesized that displacement and viscoelasticity further stimulate (or turn on the switch for) normal condylar growth by the transduction of forces over the fibrocartilage cap of the condylar head.
Dr. Bakr Rabie Faculty of Dentistry Department of Orthodontics The University of Hong Kong
Typical Effects of Functional Appliances for Class II
Posture the mandible forward
Place some distal driving force on the maxilla
Affect the vertical control of the posterior teeth (usually -Christianson effect)
Detorque the upper incisors
Torque the lower incisors forward
Have some effect on speech and esthetics (this should be a positive effect in the long run)
Do you take jaw joint x-rays before advancing the lower jaw?
It’s an important idea because it allows you to know where the condyle was before being advanced and is referenced to determine whether you are done with the functional aspect of treatment
The main result of a Class II correcting functional appliance is the remodeling of the Temporal fossa
HOW CONDYLAR MODIFICATIONS OCCUR
The growth relativity hypothesis has three main foundations:
A: The glenoid fossa promotes condylar growth with the use of orthopedic mandibular advancement therapy. Initially, that displacement affects the fibrocartilaginous lining in the glenoid fossa to induce bone formation locally.
B: This is followed by the stretch of non-muscular viscoelastic tissues
C: Third, and the most interesting aspect is the new bone formation some distance from the actual retro- discal tissue attachments in the fossa. The glenoid fossa and the displaced condyle are both influenced by the articular disc, fibrous capsule, and synovium, which are contiguous, anatomically and functionally, with the viscoelastic tissues.
HOW CONDYLAR MODIFICATIONS OCCUR
Condylar growth is affected by viscoelastic tissue forces via attachment of the fibrocartilage that blankets the head of the condyle.
Although there is some growth of the condyle, especially at the posterior aspect, the actual amount of growth of the condyle that results from the change in mandibular position is not great.


Improve Your Website
Posted by Orthodontic Products Staff | Nov 4, 2020 | Marketing and Promotion | 0

The general thought is that the more website traffic you get, the more opportunities you have to acquire patients. That is the right idea, but if they aren’t staying on your website you’ll miss out on them.
START WITH THE BASICS
Here are three easy things you can do to make sure your convert website leads.
Make sure your website has a mobile-friendly design. Everyone is on the go and on their phone, so your website needs to have full functionality on any device. Otherwise, patients may go to a more readable website.
Have your contact information conveniently located. You’ll want to provide several different ways to reach you including phone numbers, email, social media accounts, and a chat widget. It’s also a good idea to include your address and a map so they know exactly where you are.
Create a blog. Not only do blogs keep patients interested and engaged with your site, but they’re also important for their impact on Search Engine Optimization (SEO). When you insert keywords into your blogs, you’ll increase traffic that could turn into new patients.
ROUTINELY ANALYZE YOUR WEBSITE
Google Analytics is a valuable tool to help you learn about how efficient your website is performing. It’s free and can let you know how many visitors you’re getting and how they found you. Along with the tip of including keywords in your site, Google Analytics provides information on SEO performance
INCORPORATE TECHNOLOGY TO CONVERT VISITORS
You need to incorporate live chat into your website. The beneficial effects of live chats are tangible: conversions can increase by up to 20% and have a 300% ROI on sales according to the American Marketing Association.
Choose one that was created by a dentist, for dentists: Amplify. It’s an innovative way to talk to—and convert—folks visiting your site. With Amplify, a real person responds within 7 seconds no matter what time of day, in over 27 languages. It’s so innovative, it won the Cellerant Best of Class Technology Award three times.
